VIRTUAL PATIENT · CRETIC PROJECT
Artificial Intelligence
Artificial Intelligence
for clinical reasoning research.
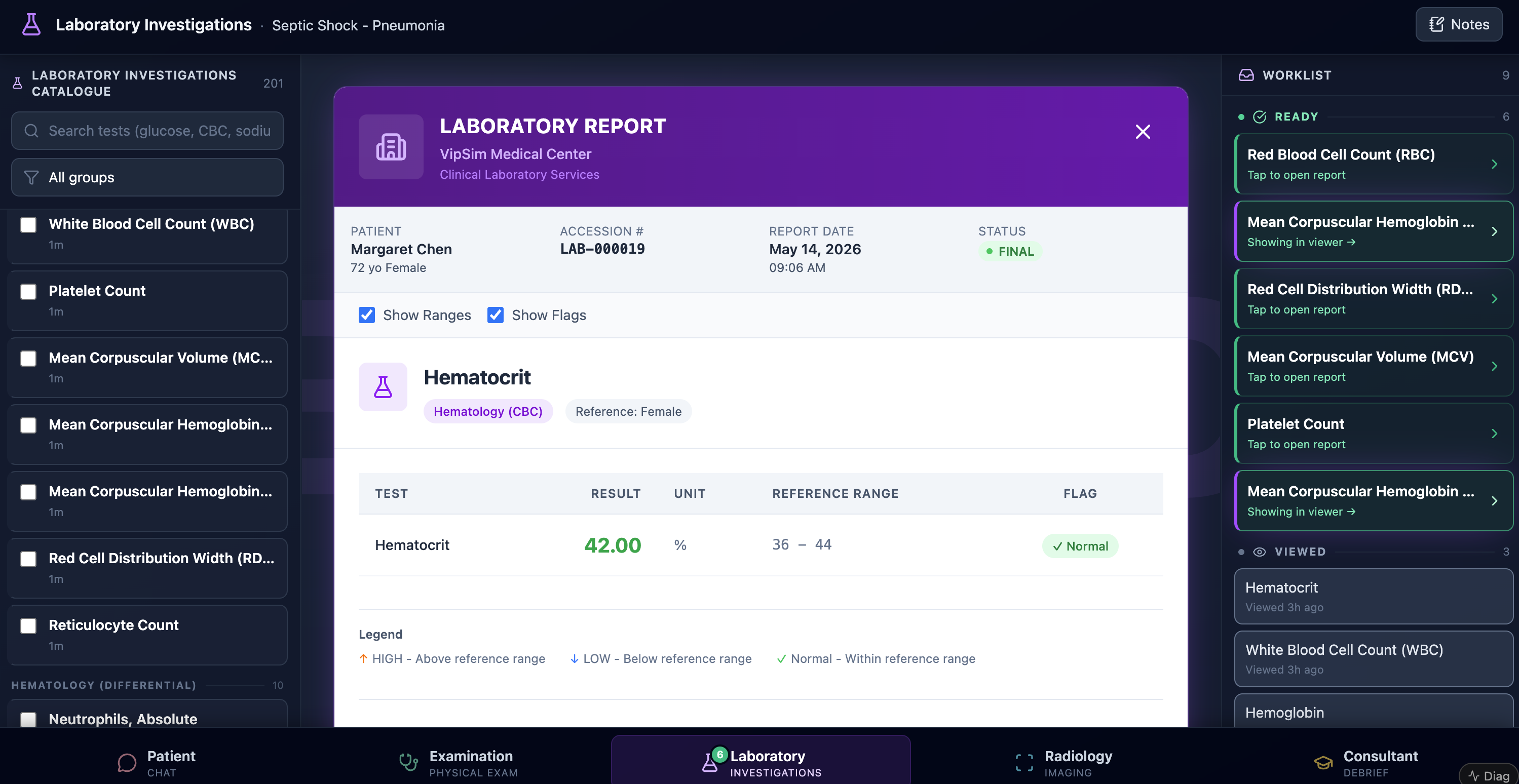
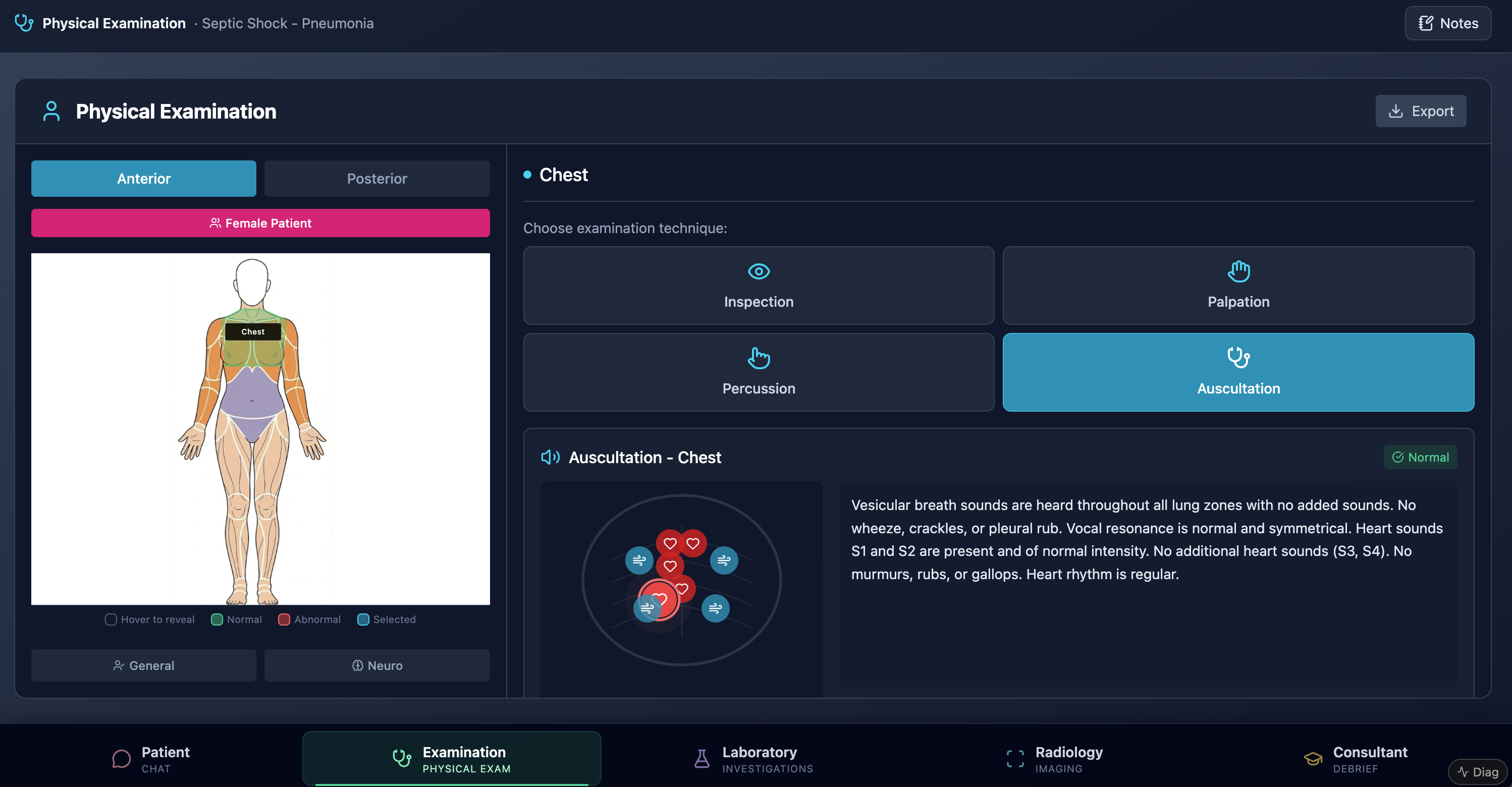
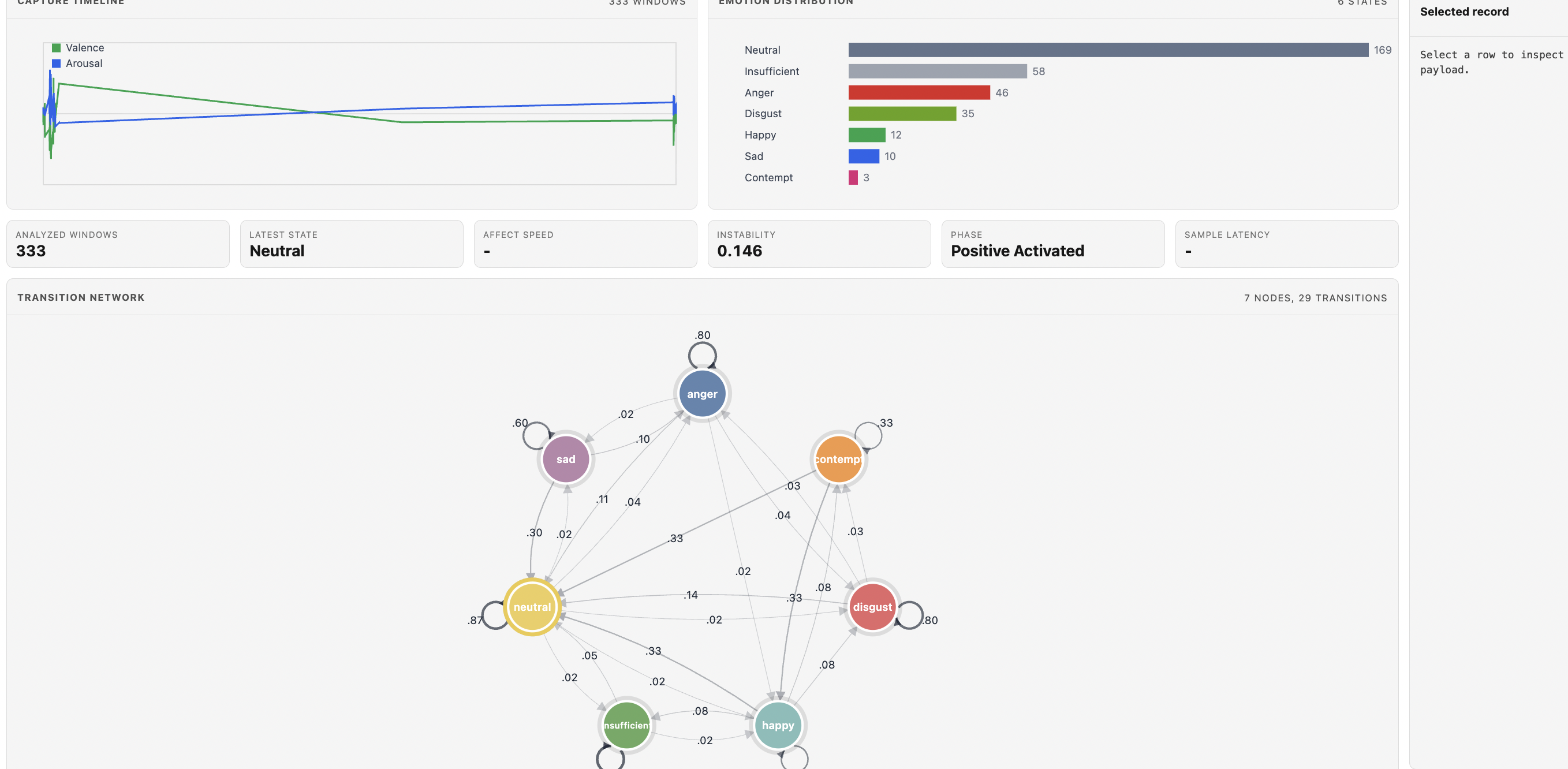
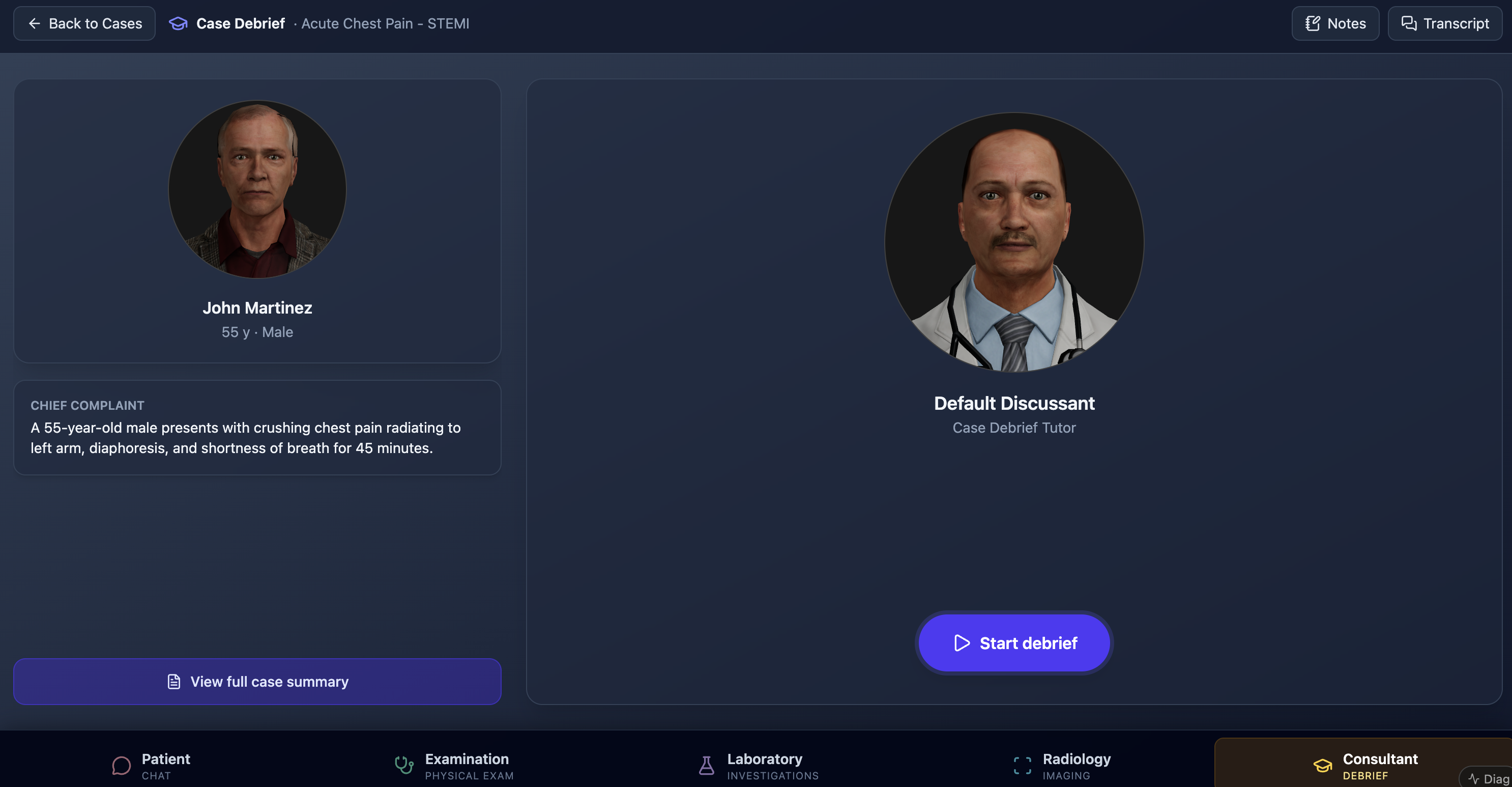
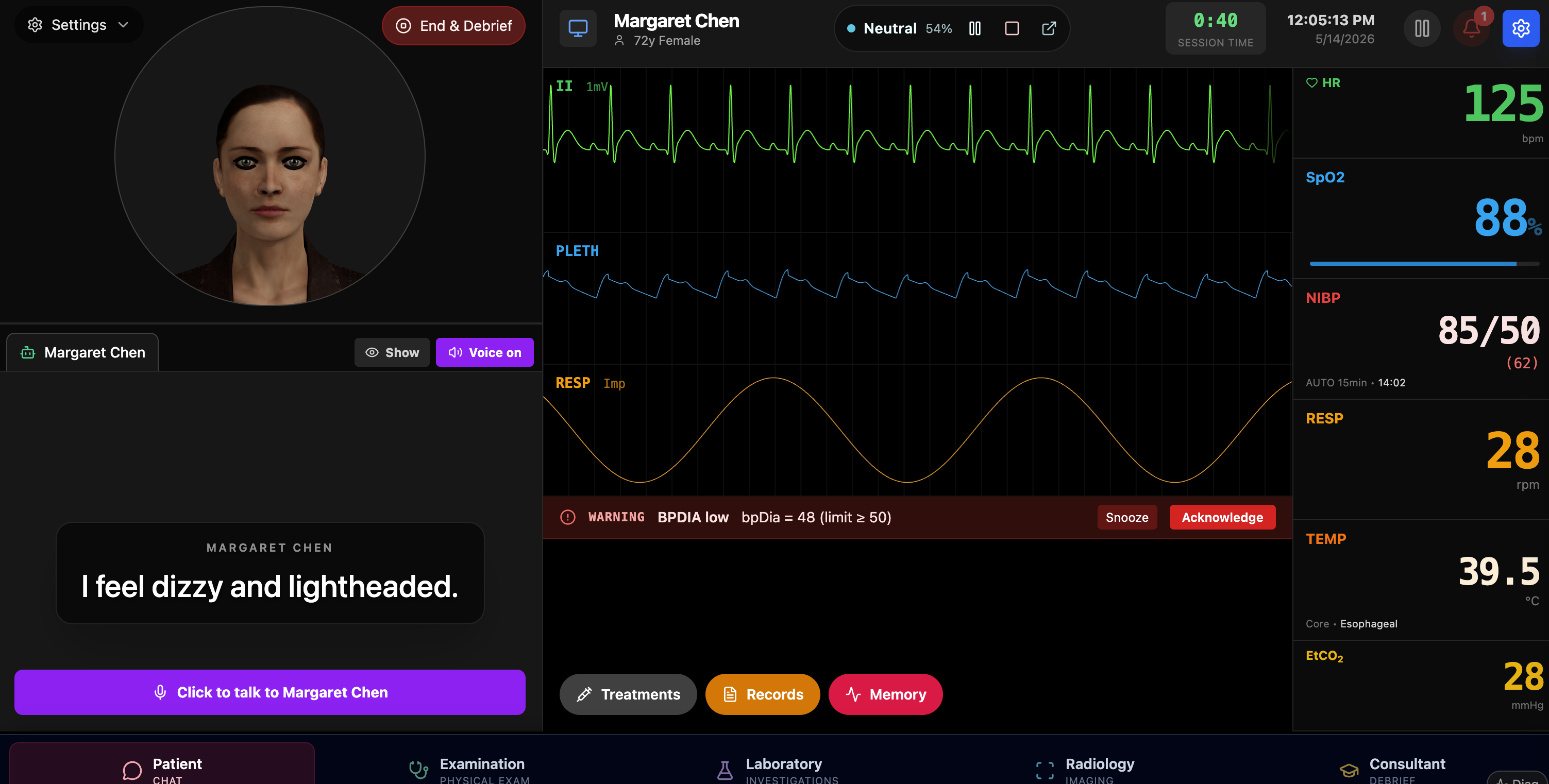
A multimodal AI-driven simulation environment. A multi-agent care team converses with the trainee; a real-rhythm physiologic monitor runs against emergency-driven scenarios with down-going trajectories; real-time affect capture and live process / sequence / transition-network analytics turn the session into a research-grade learning-analytics stream — every event row enriched with the contemporary vital signs.
AI-driven
Multi-agent
Multimodal
Real rhythm engine
Emergency scenarios
Real-time affect
Transition network analytics
Vital-enriched event log